Gum diseases, and gum inflammation in particular. are among the most common conditions in the general population, and even more so among pregnant women. Crucially, these conditions are both treatable and preventable.
In recent years, gum disease in pregnant women has been linked to a wide range of pregnancy complications, including preterm birth, low birth weight, preeclampsia, gestational diabetes, and miscarriage.
High-risk pregnancies have also been associated with numerous developmental complications in the newborn, including respiratory difficulties, motor and cognitive impairments, learning disabilities, and cardiac and metabolic disorders.
Dr. Ariel Savion has been an active dentist since 2007 and holds a dual Master’s degree from Germany in Laser Sciences and Dental Implantology. He has clinical expertise in laser periodontal therapy, microscopic surgery, and dental implant procedures.
He serves as the Medical Director of the dental corporation Savion Medical Center Ltd. and is the founder and owner of the prestigious master_implant educational club, dedicated to training dentists in advanced fields of dentistry.
In addition, Dr. Savion is the only certified instructor in Israel on behalf of the World Clinical Laser Institute in the field of laser dentistry.
Dr. Savion is an international researcher and lecturer and serves as a Key Opinion Leader (KOL) for leading medical companies in Israel and worldwide, specializing in laser dentistry, periodontology, and dental implantology.

Gum Inflammation in Pregnant Women
Gum disease is one of the most prevalent conditions worldwide. In the United States, 42.2% of adults over 30 suffer from some degree of gum disease, with nearly 8% experiencing severe cases. Among pregnant women, the figures are even more striking, certain studies estimate that approximately 70% of pregnant women experience gum inflammation to varying degrees of severity.
During pregnancy, significant hormonal shifts occur. By the end of the third trimester, progesterone levels rise to roughly ten times their baseline, and estrogen levels increase up to thirty times, far beyond what is seen during a normal menstrual cycle. Gum tissue contains receptors for these sex hormones, making it a direct target during pregnancy.
Research has confirmed a clear link between this temporary hormonal surge and both the prevalence and severity of gum inflammation. Localized gum inflammation has been found in 0.2–9.6% of pregnant women, while generalized gum inflammation affects approximately one-third of all pregnant women.
Oral Pathogens and the Pregnant Body
There are two primary mechanisms by which oral pathogens can cause harm during pregnancy. First, the pathogens themselves, or the chemicals they release, may enter the bloodstream and cause direct damage. Second, in its effort to fight these pathogens, the body produces inflammatory mediators in excess, and elevated levels of these substances can themselves be harmful.
The rising levels of sex hormones during pregnancy increase the permeability of blood vessels. Combined with gum inflammation and the bleeding it causes, this creates a pathway for oral pathogens to enter systemic circulation.
Once in the bloodstream, these pathogens, along with the chemicals they produce and the body's own inflammatory mediators, can reach the placenta and compromise its integrity, as well as the integrity of the surrounding membranes.
Indeed, studies have found a significantly higher presence of pathogens in the placentas of women with gum disease compared to those with healthy gums. Several studies have also identified a direct link between known oral pathogens and preeclampsia and hypertensive disorders of pregnancy.
Furthermore, the release of bacteria and inflammatory mediators into the bloodstream can stimulate the liver to release additional inflammatory substances, triggering whole-body inflammation. When these substances are released, they can cause intrauterine inflammation, raising the risk of preeclampsia, preterm birth, intrauterine growth restriction, and gestational diabetes.

Oral Pathogens and the Pregnant Body Gum Disease and Low Birth Weight
Low birth weight is defined as a birth weight below 2.5 kg, and very low birth weight as below 1.5 kg. Both are significant risk factors for infant morbidity and mortality in developing and developed countries alike.
The association between gum disease and low birth weight has been studied extensively. Women with gum disease face a 2 to 4 times higher relative risk of delivering a low-weight baby. A large American study involving over 1,000 women found a relative risk of 2.3 for low birth weight among pregnant women with gum disease up to week 26 of gestation, a finding that held even after adjusting for other risk factors such as age, smoking, drug use, and preeclampsia.
A study conducted in Taiwan corroborated these findings. Comparing women who delivered babies at a normal weight with those who delivered low-weight babies, the researchers found that 14.5% of the mothers in the low birth weight group had gum disease, compared to only 7.3% in the healthy group. The study further demonstrated that the more extensive the damage to gum tissue, the higher the likelihood of delivering a low-weight baby.

Gum Disease and Preterm Birth
Preterm birth is defined as delivery before week 37 of pregnancy. Early preterm birth, before week 34, which accounts for approximately 2% of all births globally, is one of the most significant causes of neonatal mortality and childhood disability.
Preterm birth carries profound health consequences for the newborn throughout life and can ultimately impose significant economic burden on the family. In most cases, preterm birth is triggered by premature rupture of the membranes surrounding the fetus.
Multiple medical studies have examined the relationship between gum disease and preterm birth, consistently finding a strong association. The relative risk ranges from 1.6 to 3.4. An American study that followed over 1,000 women up to week 26 of pregnancy, with groups stratified by the severity of gum disease and adjusted for existing risk factors, confirmed that gum disease constitutes a risk factor of 1.6 times for preterm delivery.
Gum Disease and Preeclampsia
Preeclampsia is a systemic condition characterized by high blood pressure and excess protein in the urine, typically appearing from week 20 of pregnancy onward. It affects 2–5% of all pregnant women and is one of the most significant contributors to both maternal and neonatal morbidity and mortality.
An American study examining over 1,100 participants found that women with gum disease had a 2.4 times higher risk of developing preeclampsia. A further study conducted in Korea identified an even stronger association, with a relative risk of 4.51 between gum disease and preeclampsia.
Gestational Diabetes and Gum Disease
Diabetes, and gestational diabetes in particular, is highly prevalent in the Western world. Hyperglycemia occurs in approximately 1 in every 6 pregnancies. Women who develop gestational diabetes are themselves at elevated risk of developing type 2 diabetes in the future, and the fetus is at increased risk of obesity, high blood pressure, and kidney disease.
Women with gestational diabetes are at a 2.85 times greater risk of developing gum disease. Moreover, women who suffer from both gum disease and gestational diabetes simultaneously face an 18-fold increased risk of developing preeclampsia compared to women in their first pregnancy without either condition.

Treating Gum Disease with Laser During Pregnancy
Many pregnant women suffer from chronic gum disease, yet there has historically been no truly effective solution available to them. Left untreated, chronic gum disease causes irreversible damage and poses a threat to the fetus, as described above.
The conventional approach to date involves mechanical interventions, scaling and root planing, and gum surgery with a scalpel. Laser energy offers a significant alternative: it can sterilize and eliminate the bacteria responsible for gum disease with relative ease.
Laser treatment requires no incisions or sutures and can be performed using a minimally invasive approach, without flap surgery, during pregnancy, with no risk to the mother or fetus. The patient recovers quickly and returns to daily life free of postoperative pain.
Laser can also be used to remove inflamed tissue, resurface the gums, and stimulate the regeneration of new bone and gum tissue. With laser, periodontal pockets can be reduced in depth, and teeth that would otherwise be considered "lost" can be preserved for many years.

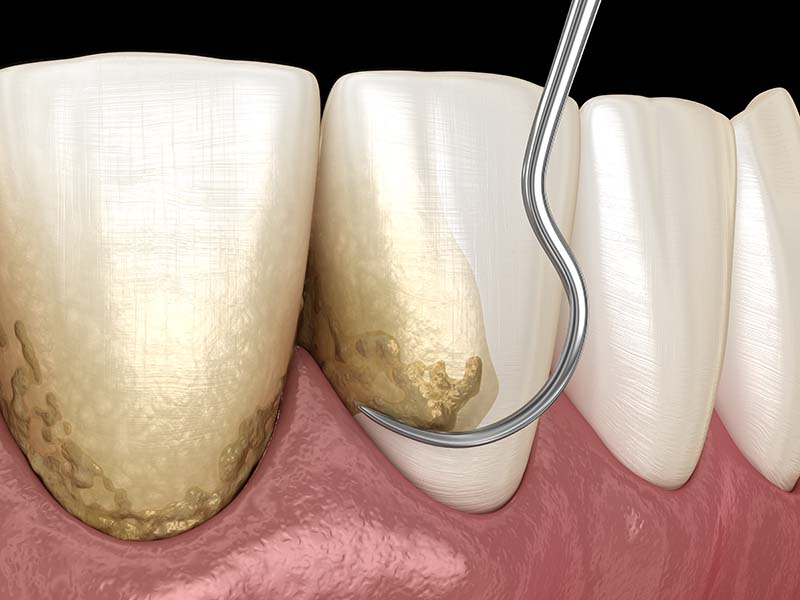
Laser Calculus Removal During Pregnancy
Another recommended treatment during pregnancy is calculus removal enhanced with laser light energy. Using a non-ablative tip, one that does not cut, the laser sterilizes and eliminates bacteria before the scaling begins, preventing the progression of chronic gum disease.
One of the key contributors to gum disease is the presence of bacteria deep within periodontal pockets. By delivering laser energy into these pockets, it is possible to effectively eliminate these bacteria and promote gum healing.
Laser treatment requires no anesthesia and is entirely painless: the light energy is absorbed by the pigment in the bacterial cell, disrupting its membrane and destroying it. This treatment is recommended for all pregnant women as a means of maintaining gum health throughout the pregnancy.
Does Laser Gum Treatment Require Specialized Training?
Professional training is mandatory before performing laser gum treatments. The oral cavity is composed of varied tissue types, and improper use of lasers on these different tissues can cause more harm than good.
Therefore, practitioners must undergo rigorous professional training on the use of different laser types and a thorough understanding of how each laser functions and its appropriate application.
Improper laser use puts both the practitioner and the patient at risk. Patients are encouraged to verify their dentist's training and certification in laser dentistry, including the specific laser types and wavelengths used.